CBT for Social Anxiety: A Practical Evidence-Based Guide
Author: Dr. Timothy Rubin, founder of Wellness AI
Originally Published: May 2026
Last Updated: May 2026

CBT for social anxiety works by changing the beliefs that keep the fear cycle going, not just by waiting out the discomfort.
Contents
- Shyness vs. Social Anxiety vs. Social Anxiety Disorder
- The Clark & Wells Model: Why Social Anxiety Persists
- Behavioral Experiments, Not Just Exposure
- Video Feedback
- Attention Training
- Dropping Safety Behaviors
- CBT vs. Medication and the Other Treatment Paths
- How Well Does CT-SAD Actually Work?
- Can You Do This on Your Own?
- Where AI Tools Fit
- A Short Note on Mindfulness
- FAQ: CBT for Social Anxiety
The most important sentence in this guide is the first one: shyness, social anxiety, and social anxiety disorder are three different things, and CBT for social anxiety was designed for the third.
About 4 in 10 American adults describe themselves as shy. Roughly 1 in 8 will, at some point in their lives, meet criteria for social anxiety disorder (SAD): a persistent, out-of-proportion fear of being judged in social or performance situations, lasting six months or more, that causes real impairment. Most popular content online blurs these together. The distinction matters. A shy person who is otherwise doing fine doesn't need a structured clinical protocol. Someone with SAD needs more than "just put yourself out there."
This guide walks through the strongest-evidence approach to treating social anxiety: Cognitive Therapy for Social Anxiety Disorder, often shortened to CT-SAD, developed by psychologists David Clark and Adrian Wells. It's a specific form of CBT, and the practical ingredients that make it work are what set it apart from generic CBT or pure exposure. If you want the broader picture first, our overview of overcoming social anxiety is a gentler starting point. This guide goes deeper into the protocol itself.
Shyness vs. Social Anxiety vs. Social Anxiety Disorder
Shyness is a temperament trait. It's common, often visible from early childhood, and not in itself a disorder. Surveys going back decades find that a large share of adults consider themselves shy at least some of the time. Shyness can be uncomfortable, but on its own it isn't impairing.
Social anxiety in the everyday sense sits one step further along. It's elevated anxiety in evaluative situations, public speaking, meeting new people, being watched while you work, that doesn't quite reach the threshold of a clinical diagnosis. It's real, and the techniques in this guide can genuinely help, but it may not need the full protocol.
Social anxiety disorder is the clinical diagnosis. The fear is persistent (six months or longer), it's clearly out of proportion to the actual social threat, and it interferes with work, school, or relationships. If you want a sense of where you fall, brief screening tools like the Social Phobia Inventory (SPIN) and the Liebowitz Social Anxiety Scale are a reasonable starting point. They don't replace a clinician's assessment, but they can tell you whether a conversation with one is worth having.
Why labor the distinction? Because full CT-SAD was built for diagnosable social anxiety disorder. Milder social anxiety often responds well to lighter-touch, self-directed versions of the same techniques. Moderate-to-severe SAD genuinely benefits from working with a trained clinician.
The Clark & Wells Model: Why Social Anxiety Persists
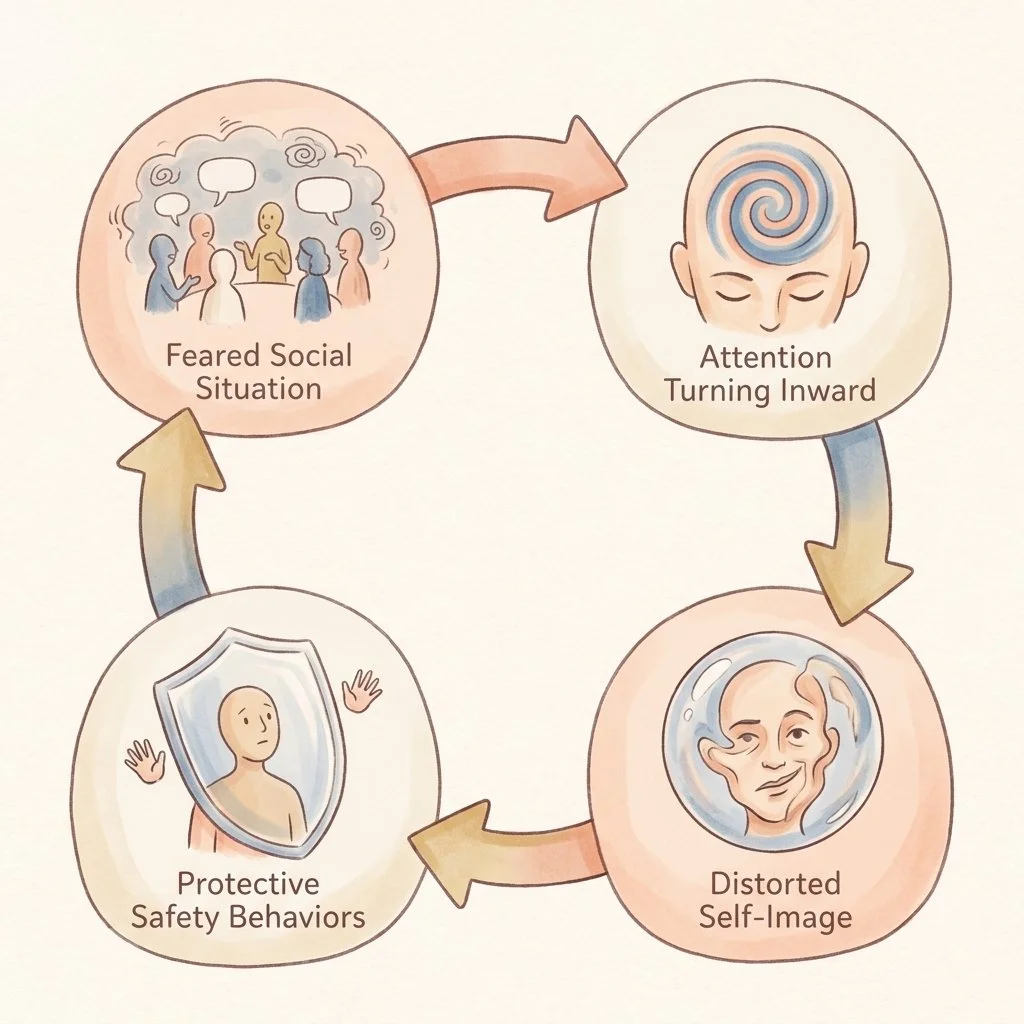
The Clark and Wells model describes social anxiety as a self-maintaining cycle, with each part open to change.
To treat social anxiety, it helps to understand what keeps it going. The Clark and Wells model, first published in 1995, is the framework most modern treatment is built on.
Picture giving a toast at a wedding. You stand up (the trigger). Old beliefs activate: "I'm boring," or "If my voice shakes, they'll lose respect for me." You start to perceive the situation as socially dangerous. From there, three processes lock the cycle in place.
The first is self-focused attention. Your attention swings inward, onto your heart rate, the tremor in your hand, the script running in your head. You stop actually noticing the people in front of you, which means you stop collecting the evidence that would tell you things are going fine.
The second is negative self-imagery. A vivid mental picture forms of how you imagine you look: red, sweating, fumbling. The trap is that you treat that internal image as fact, even though no one in the room can see what you're seeing.
The third is safety behaviors. You grip the glass to hide the shake, speak quickly to get it over with, avoid eye contact with the table you're most worried about. The catastrophe doesn't happen, but you conclude the safety behavior is what saved you, rather than learning that the catastrophe was never going to happen in the first place.
Wrapped around all of this are two more habits: anticipatory worry in the days before an event, and a post-event "post-mortem" afterward, replaying every imagined misstep. If you've ever lain awake replaying a conversation you had hours earlier, that's the post-event processing piece of this model. Studies that test the model directly find these processes account for a substantial share of social anxiety severity. The good news is that each one is also a treatment target.
Behavioral Experiments, Not Just Exposure
Here is where CT-SAD diverges from older approaches, and it's worth being precise, because this is the single most misunderstood point in social anxiety content.
Graduated exposure works on the logic of habituation: enter the feared situation enough times and the fear response gradually fades. A behavioral experiment works differently. You enter the feared situation with a specific, testable prediction, you drop the safety behaviors, and you gather actual evidence about what happens. The goal isn't to wait out the anxiety. It's to change a belief.
A prediction-based experiment sounds like this: "If I let my voice shake during the meeting, James will look uncomfortable and the conversation will end early." You then run the experiment, without the safety behavior, and check what actually happened against what you predicted. This is the same logic as cognitive restructuring, tested in the real world rather than on paper.
Why does this matter for social anxiety specifically? Because social anxiety is fundamentally a belief problem, a belief about how other people perceive you. Pure exposure can be white-knuckled through with all the safety behaviors still running, which leaves the underlying belief completely untested. In direct head-to-head trials, the Clark and Wells protocol has produced considerably larger improvements than exposure-only treatment.
Video Feedback
Video feedback is probably the most distinctive ingredient in CT-SAD, and the one most people have never heard of.
The procedure: you give a short talk or have a brief conversation that's video-recorded. Before watching, you predict in detail exactly how you think you looked, the shaking, the sweating, the awkward pauses. Your therapist coaches you to watch the recording "as if watching a stranger," setting aside how it felt at the time and assessing only what's actually visible.
Then you watch. The recording almost always shows someone far less anxious-looking than you felt. This isn't reassurance or a pep talk. It's evidence, in your own footage, that the internal self-image driving the whole cycle is simply inaccurate. The first published trial of cognitive preparation paired with video feedback found meaningful shifts in self-perception after just one session. The cognitive preparation step is what makes it land. Watching yourself without it can be far less helpful.
Attention Training

Attention training builds the skill of moving focus outward, away from internal monitoring and onto the conversation itself.
If self-focused attention is part of what keeps social anxiety going, then training attention to move is a logical target. There are two evidence-based approaches.
The Attention Training Technique, developed by Adrian Wells, is a roughly twelve-minute daily audio practice. Using competing background sounds, it trains three skills: selectively attending to one sound, switching rapidly between sounds, and attending to several at once. The aim isn't relaxation. It's strengthening your ability to deliberately unstick attention from internal monitoring.
Task Concentration Training, developed by Susan Bögels, is more situation-specific. You practice deliberately placing your attention on the conversation partner, the room, and the actual task in front of you, rather than on your own bodily sensations. It's especially useful for the performance and blushing subtype of social anxiety. Both approaches have support from controlled trials.
Dropping Safety Behaviors
Safety behaviors don't just fail to help. They frequently produce the very symptoms they're meant to hide. Gripping a glass amplifies a tremor. Over-rehearsing makes speech sound wooden. Asking a stream of deflecting questions makes a conversation feel one-sided and effortful. The performance involved can be genuinely exhausting.
CT-SAD identifies your specific safety behaviors, the conversational ones like scripting topics in advance, the performance ones like memorizing every word, the interaction ones like avoiding eye contact or sitting near the exit. Then it drops them, deliberately, inside a behavioral experiment. The repeated finding is that performance usually improves once the safety behaviors are gone, and the feared catastrophe still doesn't arrive.
CBT vs. Medication and the Other Treatment Paths
CT-SAD is the most studied protocol for social anxiety, but it isn't the only evidence-based option.
Heimberg's Group Therapy
Richard Heimberg's Cognitive-Behavioral Group Therapy is the other well-supported protocol. It runs as twelve weekly sessions in groups of around six, combining cognitive restructuring with in-session exposure through role-plays with other group members. Head-to-head, individual Clark and Wells CT-SAD tends to produce larger gains, but the group format scales better and is often easier to access. NICE guideline CG159, the UK's national treatment guidance and still the live guideline as of its May 2024 review, recognizes both models and recommends individual CBT as first-line.
Medication
NICE recommends an SSRI, specifically escitalopram or sertraline, for people who prefer medication or decline CBT. In trials that compared them directly, CT-SAD outperformed medication, and the gap tended to widen over time. This points to one of the most distinctive findings in this literature: medication benefits often fade after you stop taking it, while CT-SAD gains tend to keep improving for months after the therapy itself ends.
Beta-Blockers for Performance Anxiety
For the performance-only form of social anxiety, anxiety limited to public speaking or performing, an as-needed beta-blocker taken before the event can help with situational symptoms like tremor and a racing heart. It doesn't address the underlying beliefs. CBT does that. But as a tool for getting through a specific high-stakes performance, it has its place.
How Well Does CT-SAD Actually Work?
Well. Across the strongest trials, a clear majority of people who complete CT-SAD achieve meaningful improvement, and the effect sizes reported in meta-analyses are large. In the most recent network meta-analysis comparing psychotherapies for social anxiety disorder, the Clark and Wells protocol came out on top.
Two findings are worth holding onto. First, the gains are durable. Long-term follow-ups at one year and five years show that improvements hold up well after treatment ends. Second, as noted above, social anxiety symptoms often continue to improve in the months after CT-SAD finishes, which is not what you typically see with medication.
None of this means CT-SAD is a cure or that it works for everyone. Social anxiety is genuinely distressing, and treatment is real work. But the evidence base here is unusually deep, and it's reason for realistic optimism.
Can You Do This on Your Own?
Honestly, it depends on severity.
For mild-to-moderate social anxiety, yes, to a meaningful degree. Structured CBT workbooks and guided internet-delivered CBT both have solid evidence behind them. The two CBT-based workbooks most widely used for social anxiety, Gillian Butler's Overcoming Social Anxiety and Shyness and Antony and Swinson's The Shyness and Social Anxiety Workbook, are well-regarded and commonly used to support guided self-help. Guided online programs, which pair a structured course with brief check-ins from a therapist, can approach in-person results.
For moderate-to-severe social anxiety disorder, work with a trained CBT clinician. The ABCT "Find a Therapist" directory is a good starting point in the US. Pure unguided self-help, an app or a book with no support attached, tends to have high dropout and smaller effects, so if you go the self-directed route, build in some form of accountability.
If your difficulties extend well beyond social situations into anxiety more broadly, our guide to CBT techniques for anxiety covers the wider toolkit, and our guide to CBT for OCD covers a related long-form protocol.
Where AI Tools Fit
AI chat and meditation tools, including Wellness AI, can be a useful scaffold alongside structured CBT for social anxiety. They can help you notice and name your safety behaviors and self-focused attention, work through thought records and write-ups of your behavioral experiments, run short attention-training practices between real-world experiments, and give you a low-stakes space to think through a conversation before you have it.
What they are not is a replacement for a trained CT-SAD clinician when social anxiety is at the disorder level. An app does not formally deliver the Clark and Wells protocol, which depends on a clinician for the video feedback, the paired role-plays, and the individualized hierarchy work. The honest framing is this: use AI tools as scaffolding, not as the building.
A Short Note on Mindfulness
Mindfulness comes up a lot in conversations about anxiety, so it's worth being clear. For social anxiety specifically, generic mindfulness practiced on its own has weaker evidence than CT-SAD, and UK national guidance recommends against offering mindfulness-based interventions as a routine standalone treatment for social anxiety disorder.
The reason is mechanical, not dismissive. Social anxiety is driven by specific beliefs about how others perceive you, and changing those beliefs is what behavioral experiments are built to do. Mindfulness doesn't reliably disconfirm them. As an adjunct, something you add after the core CT-SAD work, mindfulness is perfectly reasonable. As a substitute for that core work, it's a weaker choice.
Social anxiety can feel like a fixed feature of who you are. The Clark and Wells model offers a different and better-supported view: it's a cycle, maintained by attention, imagery, and safety behaviors, and each of those is something you can change. CT-SAD is demanding, but it's one of the most thoroughly researched treatments in all of CBT, the gains tend to last, and for many people they keep growing after the work is done. If social anxiety is getting in the way of the life you want, that's a genuinely hopeful place to start.
-Tim, Founder of Wellness AI
This guide is for educational purposes and is not a substitute for professional diagnosis or treatment. If social anxiety is significantly affecting your life, consider speaking with a qualified mental health professional.
About the Author
Dr. Timothy Rubin holds a PhD in Psychology with expertise in cognitive science and AI applications in mental health. His research has been published in peer-reviewed psychology and artificial intelligence journals. Dr. Rubin founded Wellness AI to make evidence-based mental health support more accessible through technology.
Get Personalized CBT-Style Support for Social Anxiety
Wellness AI offers private, evidence-informed conversations and personalized guided meditations to support your social anxiety work between real-world steps.
FAQ: CBT for Social Anxiety
How long does CBT take for social anxiety?
National guidance recommends roughly 14 to 16 sessions over about four months for individual CBT. The Clark and Wells protocol is typically delivered in around 14 sessions of 90 minutes; the Heimberg model in around 15 weekly sessions plus a longer session for exposure work. Self-directed and internet-based formats vary, but a structured course of social anxiety treatment is generally measured in months rather than years.
Is CBT or medication better for social anxiety?
In trials that compared them directly, individual CT-SAD produced larger improvements than SSRIs. Just as importantly, CBT gains tend to keep improving after therapy ends, while medication benefits often fade once the medication is stopped. Medication, usually escitalopram or sertraline, is a reasonable option if you prefer it or decline therapy, and the two can be combined. But for durable change, the evidence favors CBT.
Can I do CBT for social anxiety on my own?
For mild-to-moderate social anxiety, yes, to a meaningful degree. Structured CBT workbooks and guided internet-delivered CBT both have solid evidence, with guided online programs approaching in-person results. For moderate-to-severe social anxiety disorder, working with a trained CBT clinician is the better path. Pure unguided self-help has higher dropout rates, so whatever route you take, build in some accountability.
What's the difference between exposure therapy and behavioral experiments?
Exposure therapy works through habituation: enter the feared situation repeatedly until the fear fades. A behavioral experiment works through belief change: enter the situation with a specific prediction, drop your safety behaviors, and gather evidence about what actually happens. For social anxiety, which is fundamentally a belief about how others see you, directly testing and disconfirming that belief is what drives most of the improvement.
What is the Clark & Wells model of social anxiety?
It's the cognitive framework most modern social anxiety treatment is built on. It describes how social anxiety is maintained by three processes once a feared situation triggers it: attention turning inward onto bodily sensations, a distorted mental self-image treated as fact, and safety behaviors that prevent you from learning the feared outcome won't happen. Anticipatory worry beforehand and post-event rumination afterward complete the cycle. CT-SAD targets each piece directly.
Does video feedback really work, and won't watching myself make me more anxious?
With proper preparation it works well. The key is predicting in detail beforehand how you think you looked, then watching the recording "as if watching a stranger." Done this way, the recording almost always shows you appearing far less anxious than you felt, which directly disconfirms the distorted self-image at the heart of social anxiety. Watching yourself without that cognitive preparation step is much less reliable.
Will the improvement from CBT for social anxiety last?
The evidence here is encouraging. Long-term follow-up studies at one and five years show that gains from CT-SAD hold up well after treatment ends. Social anxiety symptoms also often continue improving in the months after therapy finishes, a pattern that sets CBT apart from medication, where benefits tend to plateau or decline after the medication is stopped.