Cognitive Behavioral Therapy for Panic Attacks: How CBT Actually Works
Author: Dr. Timothy Rubin, PhD in Psychology
Originally Published: May 2026
Last Updated: May 2026

Panic attacks feel like an emergency, but cognitive behavioral therapy can teach you that the sensations are uncomfortable rather than dangerous.
Contents
- Panic Attacks, Panic Disorder, and "Anxiety Attacks"
- The Cognitive Model: Why Panic Snowballs
- Interoceptive Exposure: The Active Ingredient of CBT for Panic Attacks
- Cognitive Restructuring and the Safety-Behavior Trap
- How Long CBT Takes and How Well It Works
- Digital Tools and Self-Help
- When to See a Specialist
- The Takeaway
- FAQ: CBT for Panic Attacks
If you've ever had a panic attack, you know the feeling is hard to describe to anyone who hasn't. Your heart pounds, your chest tightens, the room feels unreal, and a single terrifying thought takes over: something is very wrong with me. In the moment, it can genuinely feel like a medical emergency.
Here's what decades of research have made clear, and what this guide is built around: panic attacks are intensely uncomfortable, but they are not dangerous. And cognitive behavioral therapy for panic attacks is the most effective, best-studied way to break free of them.
This guide goes deeper than "try deep breathing." We'll walk through how CBT for panic actually works, why a technique called interoceptive exposure is considered the real engine of recovery, and one important nuance most articles get wrong: how breathing exercises can quietly keep panic going if you use them the wrong way.
Panic Attacks, Panic Disorder, and "Anxiety Attacks"
These terms get used interchangeably, but the distinction matters for understanding how CBT helps.
A panic attack is an event: a sudden surge of intense fear that peaks within minutes, paired with physical symptoms like a racing heart, shortness of breath, dizziness, chest pain, trembling, or a feeling of unreality. Panic attacks are surprisingly common. Many people have one or two during stressful periods and never have another, and they can show up alongside many different conditions.
Panic disorder is a condition. It's diagnosed when someone has recurrent, unexpected panic attacks plus persistent worry about having more of them, or changes their behavior to avoid them. According to the National Institute of Mental Health, panic disorder affects a small but significant share of adults. The key feature is the fear of the fear itself.
You may also hear the phrase "anxiety attack." It's a common everyday term, but it isn't a formal diagnosis. People usually mean a build-up of anxious distress that's milder and more gradual than the sudden spike of a true panic attack.
Why This Distinction Shapes CBT
CBT for panic attacks doesn't really aim to stop the attacks one by one. It targets the cycle that turns isolated attacks into an ongoing disorder: the catastrophic fear of the sensations, and the avoidance that fear creates.
Understanding that shift, from "stop the attack" to "remove the fear of the attack," is the foundation of everything that follows.
The Cognitive Model: Why Panic Snowballs
Modern CBT for panic rests on a model proposed by psychologist David Clark in his influential 1986 paper on the cognitive approach to panic. It explains panic with one core idea: panic attacks result from the catastrophic misinterpretation of normal bodily sensations.
In plain terms, your body produces a sensation, and your mind reads it as a disaster. A racing heart becomes "I'm having a heart attack." Dizziness becomes "I'm about to collapse." Breathlessness becomes "I can't breathe, I'm going to suffocate."
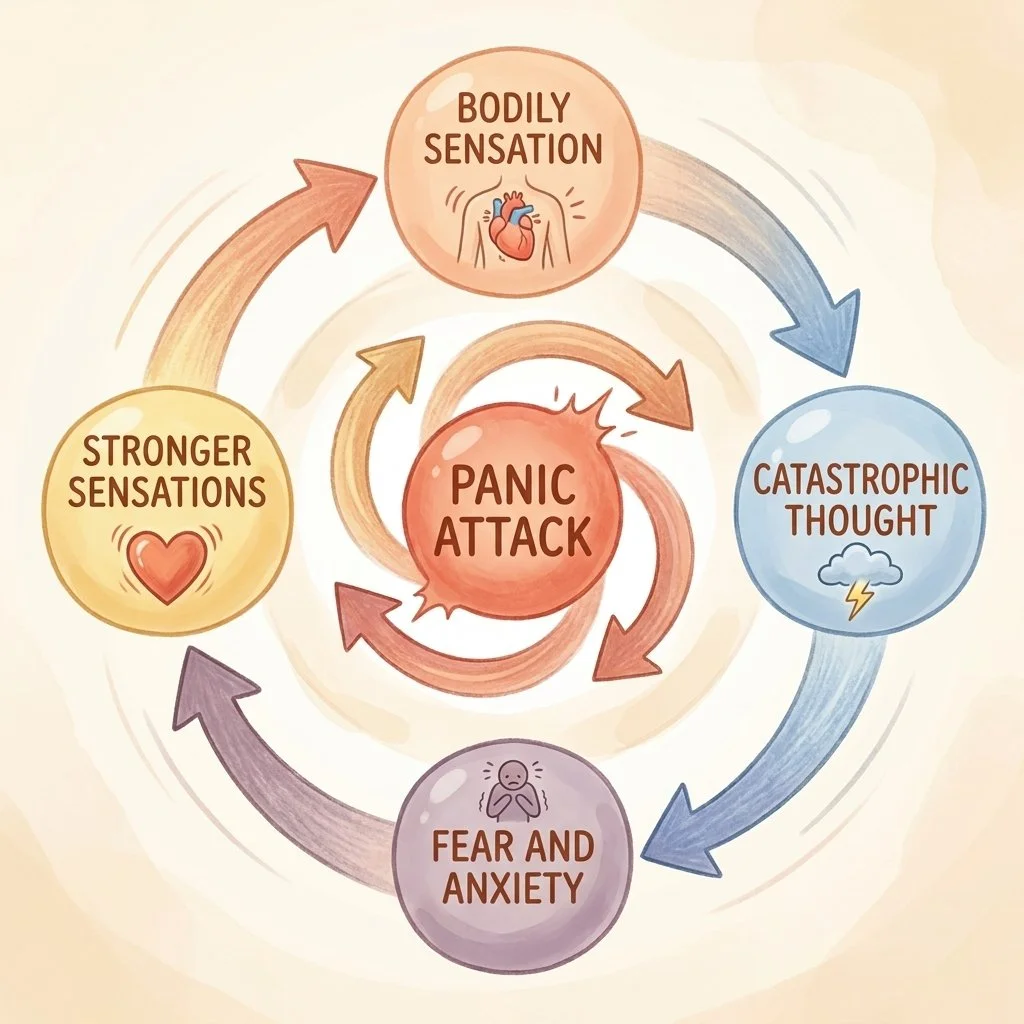
The panic cycle: a bodily sensation is misread as dangerous, which produces fear, which intensifies the sensation, looping into a full attack.
Here's the trap: that frightening interpretation produces more fear, and fear produces more of the very sensations you're afraid of. Stronger sensations seem to confirm the catastrophe, which cranks up the fear again. It's a feedback loop that can spiral into a full panic attack in seconds.
This also explains panic that seems to come "out of the blue." The trigger is often just a harmless internal sensation, from caffeine, exercise, heat, or a normal flutter, that you didn't consciously notice before your mind flagged it as a threat.
The encouraging implication of Clark's model is that because panic is maintained by misinterpretation, it can also be corrected. That's exactly what CBT sets out to do.
Interoceptive Exposure: The Active Ingredient of CBT for Panic Attacks
If there's one part of this guide to remember, it's this section. When researchers have taken CBT for panic apart to see which pieces do the heavy lifting, one technique consistently stands out: interoceptive exposure.
A large analysis of dozens of treatment studies in Psychological Medicine compared the individual components of CBT for panic. Interoceptive exposure was the component most strongly linked to the best results. Tellingly, two programs could both be called "evidence-based CBT" while differing dramatically in effectiveness, depending on whether they included this technique.
What Interoceptive Exposure Actually Is
Interoceptive exposure means deliberately bringing on the physical sensations of panic, on purpose, in a safe and planned way. It sounds counterintuitive, even alarming. Why would you want to feel those things?
Because avoiding them is what keeps panic alive. When you repeatedly create the feared sensations and nothing catastrophic happens, you learn something your anxious mind couldn't accept in theory: these sensations are uncomfortable, but harmless. Clinicians sometimes describe the goal as removing the "fear of fear."
The Standard Exercise Menu
With a therapist, you'd typically work through a set of short exercises, each designed to reproduce a particular cluster of sensations:
- Overbreathing for about a minute, to produce dizziness, tingling, and unreality
- Breathing through a thin straw with your nose pinched, to create air-hunger and chest tightness
- Spinning in a chair, to bring on lightheadedness
- Running in place or up stairs, to produce a racing heart and breathlessness
- Holding your breath, to create chest tightness
- Shaking your head side to side, to produce disorientation
- Staring at a bright light or at yourself in a mirror, to bring on feelings of unreality
These are repeated and structured, not random. You and your therapist build a ranked list of exercises from least to most distressing, rate your distress on a simple 0-to-100 scale, and work upward, repeating each one until it loses its grip.

Interoceptive exposure is practiced gradually and structured, starting with milder exercises and working upward step by step.
Why It Works: Learning That Surprises You
For years, the explanation was "habituation", the idea that anxiety simply fades as you stay with it. But the more current and useful explanation comes from the inhibitory learning model, developed by psychologist Michelle Craske and colleagues in their work on maximizing exposure therapy.
The key word is surprise. You go into an exercise holding a prediction: "If my heart pounds this hard, I'll pass out." The exercise creates a mismatch. Your heart pounds, and you don't pass out. That gap between what you feared and what happened builds a new "this is safe" memory that competes with the old fear.
This reframes the goal in an important way. The point of an interoceptive exercise is not to feel calm by the end. It's to be surprised that nothing bad happened. Feeling better during the exercise is nice, but the learning is what lasts.
Facing Feared Places, Too
Interoceptive exposure handles feared sensations. Many people with panic disorder also develop agoraphobic avoidance, steering clear of places where escape or help feels hard, like crowded stores, public transit, highways, or being far from home.
CBT pairs interoceptive work with in-vivo exposure: gradually, deliberately re-entering those avoided situations. The two work together to give you back the parts of life that panic had quietly shrunk.
Cognitive Restructuring and the Safety-Behavior Trap
Alongside exposure, CBT works directly on those catastrophic thoughts, a process called cognitive restructuring. This is closely related to the thought-reframing techniques used for anxiety more broadly.
Questioning the Catastrophe
Rather than arguing yourself out of fear, you examine the scary thought as a hypothesis. How many panic attacks have I had? How many heart attacks? Is a racing heart actually dangerous, or just adrenaline doing its job?
You also practice decatastrophizing, following the feared chain to its realistic end: even at its worst, a panic attack means feeling awful for a few minutes, not collapsing or dying. The most powerful tool here is the behavioral experiment, where you test a belief rather than just discussing it. In practice, this is what an interoceptive exercise is.
When Breathing Becomes Part of the Problem
Here's the nuance most guides miss. Slow, deep breathing feels like the obvious answer to panic, and it's taught everywhere. But the research is genuinely cautious about it.
A controlled study in the Journal of Consulting and Clinical Psychology compared CBT for panic with and without breathing retraining. Adding breathing techniques produced no extra benefit, and some results pointed to slightly worse outcomes.
Why? Because breathing can quietly become a safety behavior, something you do to prevent a feared catastrophe. If you breathe slowly to stop yourself from suffocating or losing control, and then nothing bad happens, you credit the breathing, not the fact that the sensation was never dangerous. The catastrophic belief never gets disproven, and the crutch keeps the fear standing.
The point isn't "never breathe slowly." Breathing exercises are genuinely useful for general, everyday anxiety. The trap is using them as a panic off-switch. If you're drawn to breathwork, our guides on breathwork for anxiety and grounding techniques for panic attacks can help, with one caveat to carry with you: use these as ways to relate to anxiety, not as rituals to block panic. In panic disorder, real recovery comes from letting an attack rise, crest, and pass on its own.

Safety behaviors feel protective, but they quietly prevent your brain from learning that the feared sensations were never dangerous.
Other Safety Behaviors Worth Dropping
Breathing isn't the only crutch. Common safety behaviors that quietly maintain panic include:
- Carrying anti-anxiety medication "just in case," even if you rarely take it
- Always sitting near exits or choosing aisle seats
- Checking your pulse or scanning your body for symptoms
- Needing a "safe person" with you to go places
- Avoiding caffeine, exercise, or heat because they mimic panic sensations
- Mentally rehearsing escape routes wherever you go
Each one sends your brain the same message: that situation was dangerous, and the crutch saved me. Genuine recovery means doing the feared thing and gradually letting the crutch go.
How Long CBT Takes and How Well It Works
One of the most reassuring things about CBT for panic is that it's designed to be short. The American Psychiatric Association's guideline describes it as a time-limited treatment, generally around 10 to 15 weekly sessions. The UK's NICE guideline similarly frames it as a course completed within a few months.
CBT is recommended as a first-line treatment for panic disorder by both NICE and the APA, on par with medication. For many people who complete it, it leads to becoming panic-free.
The Lasting-Results Advantage
The standout finding is about durability. Because CBT teaches you transferable skills, its benefits tend to hold after treatment ends. A review of long-term outcomes in JAMA Psychiatry found relatively low relapse rates after successful CBT for anxiety disorders.
Medication, by contrast, works well while it's being taken, but relapse is common after it's stopped. This isn't an argument against medication, which is an effective, legitimate choice that many people use alongside therapy. It's simply why CBT has a unique edge: the skills stay with you. CBT can even make it easier to come off medication later, by lowering relapse risk during that transition.
Digital Tools and Self-Help
Not everyone can access a CBT therapist right away, and there's good news here. Guided self-help and structured internet-delivered CBT for panic have a solid evidence base, and NICE endorses low-intensity options as a sensible first step. Working through a CBT-based workbook or program is a legitimate starting point, not a lesser one.
This is also where digital mental health tools fit. Apps like Wellness AI can help you practice CBT-informed skills, build awareness of the panic cycle, and reflect on anxious thoughts between or instead of formal sessions.
It's worth being clear about what such a tool is and isn't: most apps do not provide formal, structured Panic Control Treatment, and it isn't a replacement for a trained CBT therapist if your panic is moderate to severe. Used realistically, though, digital tools can widen access and support the day-to-day work of recovery.
If you'd like a broader foundation in the techniques behind all of this, our pillar guide on CBT techniques for anxiety is a good companion to this one.
When to See a Specialist
Self-help is a strong first step, but interoceptive exposure, the active ingredient, is also the part people most often avoid or do half-heartedly on their own. Because avoidance is the disorder, that matters.
Consider working with a trained CBT therapist if your panic is severe or frequent, if agoraphobic avoidance is shrinking your daily life, if you're also dealing with depression, trauma, or substance use, or if self-help hasn't moved the needle within a reasonable window. Reaching out for that help is a sign of good self-care, not failure.
Rule Out Medical Causes First
One important caveat: before treating recurring panic as panic, see a doctor once to rule out physical conditions that can mimic it, particularly thyroid and cardiac issues. This is a one-time step.
Once you've been checked and reassured, resist the urge to keep seeking medical reassurance, because repeated checkups and ER visits can themselves become safety behaviors. Get evaluated once, trust the result, and then do the CBT work with confidence.
The Takeaway
Panic attacks convince you that your body is dangerous. Cognitive behavioral therapy for panic attacks works by patiently proving otherwise, not with reassurance, but with direct experience.
Interoceptive exposure teaches you, in your own body, that the sensations you fear can't actually hurt you. Cognitive restructuring loosens the catastrophic thoughts. And dropping safety behaviors, including the well-intentioned habit of "controlling" your breathing, lets the fear finally run out of fuel.
It takes courage, and usually it takes guidance. But panic disorder is one of the most treatable conditions in mental health, and the freedom on the other side is real and lasting.
-Tim, Founder of Wellness AI
About the Author
Dr. Timothy Rubin holds a PhD in Psychology with expertise in cognitive science and AI applications in mental health. His research has been published in peer-reviewed psychology and artificial intelligence journals. Dr. Rubin founded Wellness AI to make evidence-based mental health support more accessible through technology.
Practice CBT Skills for Panic and Anxiety
Try Wellness AI for guided, CBT-informed support and personalized meditations to help you understand and ride out anxiety.
FAQ: CBT for Panic Attacks
Is cognitive behavioral therapy effective for panic attacks?
Yes. CBT is recommended as a first-line treatment for panic disorder by both NICE and the American Psychiatric Association, and many people who complete it become panic-free.
How long does CBT for panic attacks take?
It's a short, time-limited therapy, typically around 10 to 15 weekly sessions, with briefer and more intensive formats also available.
What is interoceptive exposure?
It's a CBT technique where you deliberately bring on the physical sensations of panic, such as a racing heart or dizziness, in a safe and structured way, so you learn firsthand that they're uncomfortable but not dangerous.
Are panic attacks dangerous?
No. A panic attack is your body's alarm system firing when there's no real threat. It feels frightening, but it cannot harm you, and it always passes on its own.
Can deep breathing make panic worse?
It can, if you use it to "prevent" a feared catastrophe. Used that way, breathing becomes a safety behavior that stops you learning the sensations were never dangerous. As a general tool for everyday anxiety, breathing exercises are still helpful.
Is CBT better than medication for panic attacks?
Both are effective and can be used together. CBT's main advantage is durability, because it teaches lasting skills, its benefits tend to hold after treatment ends, while relapse is more common after stopping medication.
Can I treat panic attacks on my own?
Guided self-help and internet-delivered CBT have good evidence and are a reasonable first step for mild to moderate panic. Severe or frequent panic, or significant avoidance, is best addressed with a trained CBT therapist.
Should I see a doctor about my panic attacks?
Yes, once. A single medical check rules out conditions like thyroid or heart problems that can mimic panic. After that, repeated reassurance-seeking can become a safety behavior, so it's best to trust the result and focus on treatment.